We are honored to receive the Newcomer of the Year Industry Award at ECR 2025. Our congress team (from left to right): Conny Schueller, Gerd Schueller, Jimmy Beständig, Andrea Rockall, Michael Peck, Aferdita Bogdanovic, Markus Lang
Was the European Congress of Radiology ECR 2025 our success? How can we understand and evaluate success as an exhibitor at a medical congress? Is it because we conducted countless contract negotiations? Is it because we made money? All of them, no!
Our success with ERS and Radailogy goes beyond business figures
ERS and Radiology have been recognized as trendsetters who always puts people’s well-being first. We offer our teleradiology and artificial intelligence to quickly and clearly give people the reassurance they need to make important decisions immediately:
Can I go home from the doctor’s office without treatment, allowing me to continue my life with joy and serenity without worry? Or is my decision to seek treatment now the better one for quickly regaining my health? Above all, I don’t have to worry about any unclear information about whether my medical report might mean that no one knows for sure whether my health is at risk or not.
We apply all our knowledge to enable these very decisions, every day of the year, for people all over the world
We have become the market leader in teleradiology not only because our customers rely on our clear decisions.
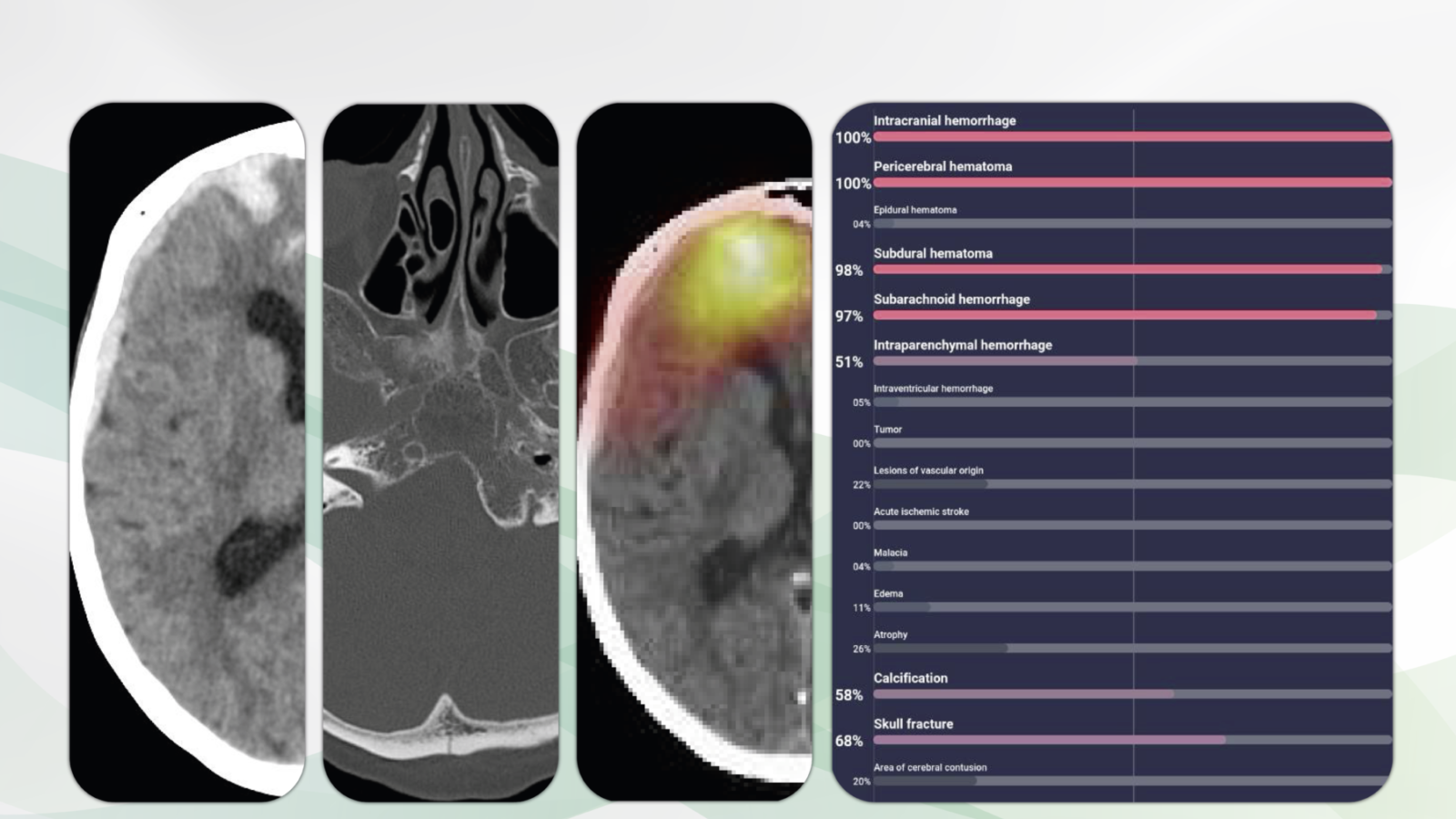
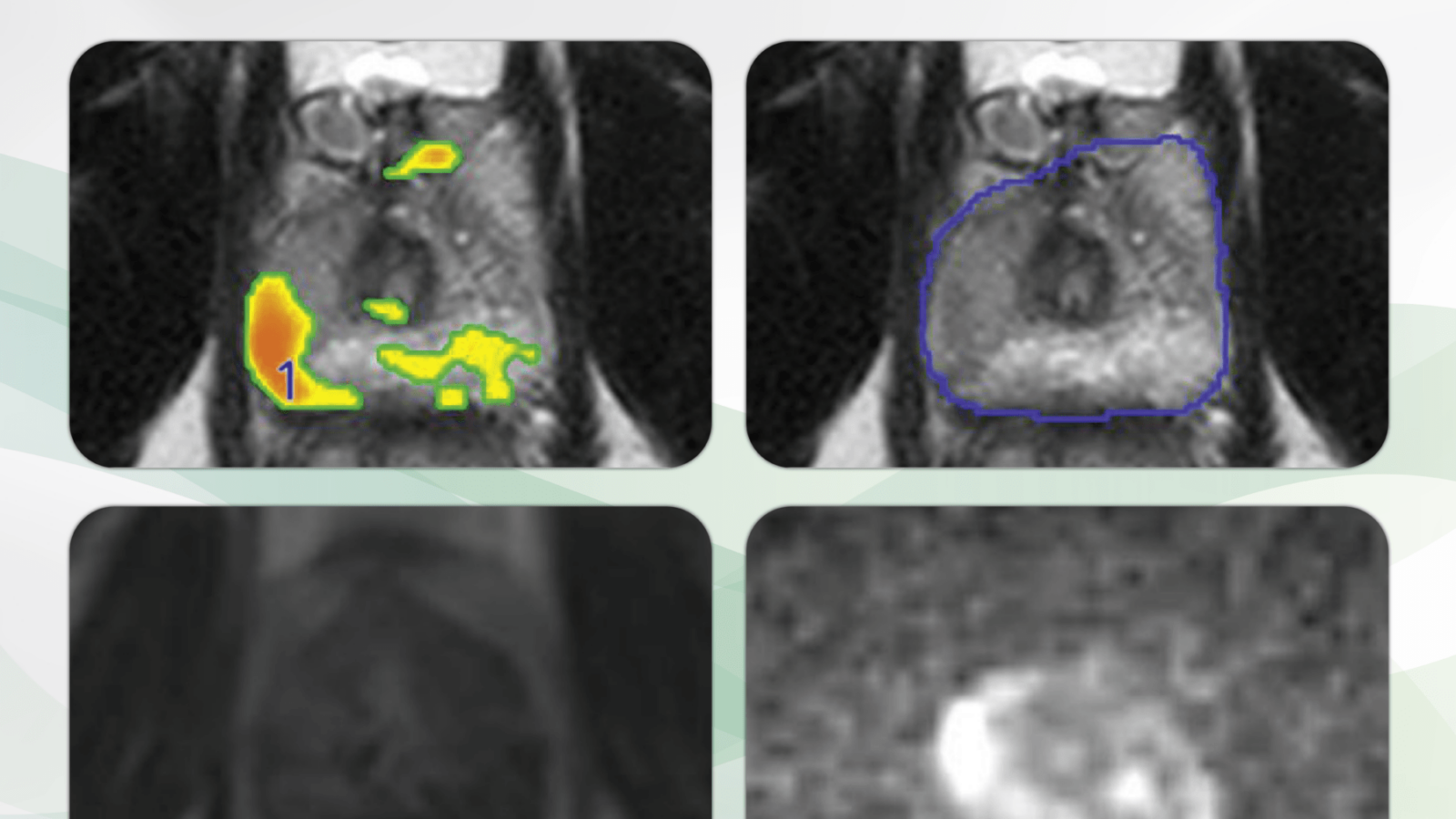
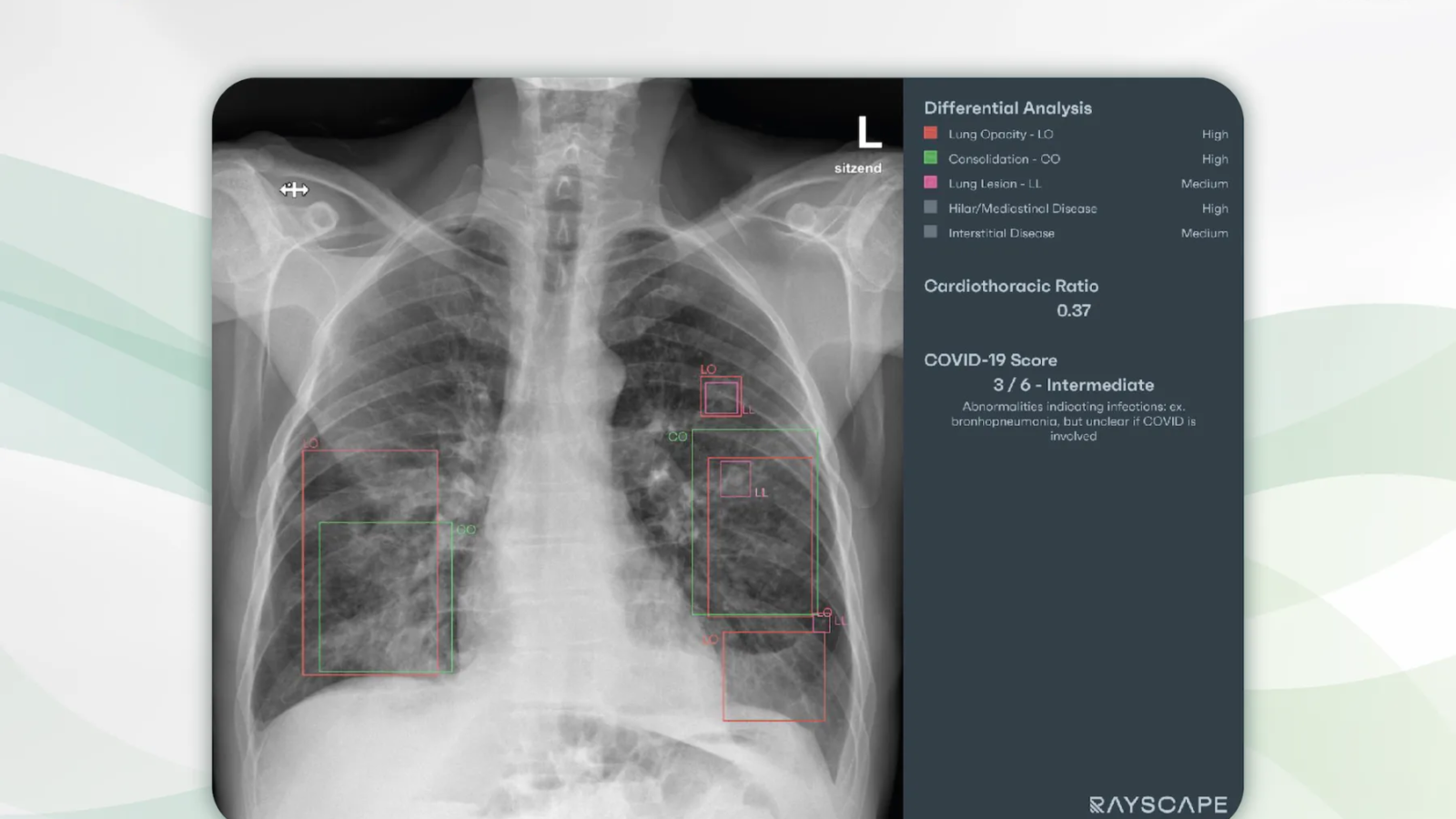
With Radailogy, we implement additional machine results with great care and diligence. And it is precisely at this interface that it is crucial to carefully review the AI assistant’s results for each individual and integrate them into our human responsibility, i.e., our medical reports.
We conveyed these human values. That´s what it´s all about. That´s what our success is all about
ECR 2025 has shown that our unique path is also the only right one. Thank you to everyone who helped make our participation in ECR 2025 in Vienna such a wonderful celebration.
Yours,
Gerd Schueller